


It would be criminal and somewhat sacrilegious if we failed to bring up the topic of football (or "soccer" as our American friends call it), in this most hallowed of seasons for the sport’s fans all over the world. Especially in a country like our own, people have this one-month to escape the poverty, injustice and misfortunes of their reality in the ecstasy that is - the world cup.
And when Discussing the world cup, it would be blasphemous, as Ethiopians, if we fail to remember Mr.Yidnekachew Tessema (Father of African sports). If it were not for this pioneering individual Africa would still be sending only two teams to the world cup.
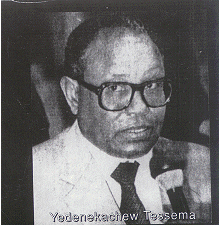
Yidnekachew's football career began in his teens. In the mid 1930s, he was one of the founding members of the St. George soccer club. As a post-war government-appointed sport official, Yidnekachew helped promote soccer as a popular national pastime by helping found new teams and arranging matches in different parts of the country. His efforts paid off in 1953 with FIFA's acceptance of Ethiopia as its fourth African member after Egypt (1923), Sudan (1948) and South Africa (1952).Having represented his country at the CAF formation conference in Sudan, in 1961 Yidnekachew was chosen as the organization's vice president. A decade later, he replaced the Egyptian Abdel Aziz Salem as CAF's president, a position he held until his death in August 1987. (Fikru Gebrekidan, Seleda)
The Nigerian Olu Amadasun, writer of the book , History of Football in Africa comments, "It would not be immodest to say that apart from being one of the founding fathers of CAF, he (Yidnekachew) has been the author of all the African proposals submitted to the FIFA congress several of which have meant modification of the statutes, Yidnekachew, championed tirelessly Africa's interest especially that which compelled FIFA to grant Africa an additional spot in the 1982 World Cup."
Major organizations with which Yidnekachew was closely associated included the Federation of International Football Association (FIFA), the International Olympic Committee (IOC), the Union of African Sports Olympic Committees Association and the Supreme Council for Sports in Africa. Yidnekachew's contribution to the development of sports in Africa has earned him international awards and recognition. In 1978, the newly introduced African Youth Championship Cup was named in his honor: Tesemma Cup. Other tributes, according to Amadasun, included an honorary medal by the African Union of Sports Journalists and a sport merit medal by the Zairian government. He was also conferred knighthood by the Ivorian government, a perfect irony for a citizen whose Marxist government espoused the gospel of universal proletarianism. (Fikru Gebrekidan, Seleda)
Yidnekachew passed away on August 20, 1987, after a long battle with cancer. Yidnekachew’s death was a major loss not only for Ethiopia but for the entire continent of Africa as well.
Rest in Peace.
Continuing on this theme of the World cup,
We have for you today a video of Diego Armando Maradona, arguably the most talented football Player to ever walk this planet.
The Mexico 86’ world cup showcased Maradona’s ability to an astounded world, and produced many memorable matches still highlights in world cup history. The match between Argentina and England was one such moment. This match is remembered for two reasons, “The hand of God” and “The Greatest Goal in FIFA World Cup History”.
The first is Maradona’s controversial (dare we say artistic?) illegal Hand goal. And the second, a moment of pure magic, in which Maradona demonstrated his unparalleled dribbling skill. FIFA voted this goal in 2002 as “the goal of the century”. Nine minutes into the second half, Enrique passed the ball to Maradona some ten meters inside his own half. Maradona then began his 60 meter, 10 second dash towards the English goal, dodging five English outfield players as well as goalkeeper Peter Shilton to make the score 2-0 to Argentina. English striker Gary Lineker later said "[it was] probably the one and only time in my whole career I felt like applauding the opposition scoring a goal." A statue of Maradona immortalizing the moment has been erected outside the stadium.
Enjoy!
Watch in slow-motion
.







































{kind=link}
{kind=link}
{kind=link}